


Read more
Blog, Public Attitudes
Making the ‘Movable’ Middle More Open to Immigration
For those working to promote a positive and more balanced view about migration in high-income countries, the world can seem a bleak place at times. From drownings in the Mediterranean, to detention centres in...
Severe shortages of health personnel provide a justification for the international community to support developing countries in their efforts to retain medical workers through improved local conditions. Our new research shows that aid for health as well as general efforts to foster economic growth indeed lead to lower emigration of medical workers. The effects are modest, however, suggesting that foreign assistance can only play a minor role in mitigating the medical brain drain.
Concerns about medical brain drain
Debates on the extent to which developing countries suffer from a brain drain often focus on the emigration of locally scarce health personnel. The emigration of high-skilled workers in general, and medical workers in particular, can be considered as a loss of human capital, often (although perhaps not always) negatively influencing the welfare of those who remain in the source countries (e.g. Adovor et al 2021; Bhagwati and Hamada 1974).
Over 40 percent of Member States of the World Health Organisation (WHO) report to have fewer than 10 medical doctors per 10,000 population, and over 55 percent report to have fewer than 40 nursing and midwifery personnel per 10, 000 population (WHO 2020). To put this into perspective, the corresponding OECD averages are 35 (for medical doctors) and 96 (for nurses), respectively. Empirical studies have shown that the emigration of doctors is associated with high HIV death rates; child mortality; and an insufficient number of medical workers to meet local health care needs, pointing to a medical brain drain (see Chauvet et al. 2013; Bhargava and Docquier 2008; Astor et al. 2005). The existing research literature also points to instances where emigration prospects for medical workers provide incentives for investment in education that are sufficiently high to bring about a net welfare gain for the country of origin (e.g. Abarcar and Theoharides 2020; Kangasniemi et al. 2007).
Irrespective of whether there is a brain drain or a brain gain, there are likely to remain considerable shortages of health personnel that could give rise to large welfare losses, particularly in poor and deprived areas and under challenges such as the COVID-19 pandemic. Against this background, we argue that there is a justification for the international community to support developing countries in their efforts to retain medical workers through improved local conditions. Recent empirical evidence suggests that the emigration of physicians is negatively affected by rising levels of economic development at the origin and by higher levels of health aid (Adovor et al 2021; Moullan 2013). Hence, efforts of foreign aid donors to create development opportunities at the local level could lead to lower emigration rates of medical workers.
At a theoretical level, this finding is not necessarily inconsistent with the well-known inverted-U-shape hypothesis about the relationship between emigration rates and development (see Zelinsky 1971). The logic behind this hypothesis is as follows: At low levels of development, additional income is likely to enable a larger share of the population in the countries of origin to finance migration costs, raising the number of people who leave. At higher development levels, the fact that rising domestic incomes provide an incentive to stay becomes more important than budgetary constraints that prevent people from emigrating. Physicians are an upper socio-professional occupation in developing countries, both financially and educationally. Compared to people working in lower-income occupations, physicians in developing countries can more easily afford the costs of migrating abroad and face lower income gains from moving and taking up employment in high-income countries. Hence, physicians are likely to lie on the downward-sloping segment of the inverted U-curve.
New research: Foreign aid reduces emigration of both doctors and nurses
In our recent Working Paper (Lanati and Thiele 2020), we go one step further and explore the effect of per-capita income and health aid on the emigration of medical workers to OECD countries by adopting a broader definition of medical brain drain which includes not only doctors but also nurses. Nurses are poorer than doctors and more likely to be located on the upward-sloping part of the inverse u-curve. As shown in Figure 1, the United States is clearly ahead of all other OECD countries as the main destination for nurses (44 percent of foreign-born workers in the OECD) as well as doctors (36 percent of foreign-born workers in the OECD).
Our estimates show that additional health aid and higher GDP per capita are both associated with lower emigration for both groups of medical workers, which points to the absence of an inverted u-curve as even nurses are less likely to leave in response to better local conditions. We also shed light on the key mechanisms through which aid for health is likely to affect the incentives of medical workers to emigrate from developing countries. Our findings suggest that sector-specific foreign assistance leads to improvements in the quality of health infrastructure, which in turn influence medical workers’ migration decisions.
Modest effects
From a development policy perspective, our findings imply that foreign assistance targeted at improving health infrastructure can help mitigate the medical brain drain. The same is true for more general efforts by the international community and local governments to raise growth prospects. It has to be noted, however, that our estimates point to quantitatively modest impacts and therefore suggest only a minor role for development-oriented measures in reducing the emigration of medical workers from low-income countries.
The Working Paper is available for download here
Figure 1: Distribution of foreign-born doctors (Left) and nurses (Right) by Country of Residence in the OECD, 2010/11
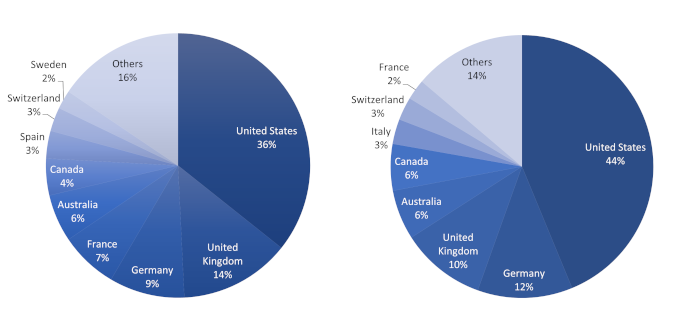
Source: DIOC 2010/11, LFS 2009/12. OECD International Migration Outlook 2015
References
Abarcar, P., and C. Theoharides (2020). Medical Worker Migration and Origin-Country Human Capital: Evidence from US Visa Policy. SocArXiv Papers, August, 3.
Adovor, E., M. Czaika, F. Docquier, and Y. Moullan (2021). Medical Brain Drain: How Many, Where, and Why? Journal of Health Economics 76: 102409.
Astor, A., Akhtar, T., Matallana, M. A., Muthuswamy, V., Oluwu, F.A., Tallo, V., and Lie, R. K. (2005). Physician migration: Views from professionals in Columbia, Nigeria, India, Pakistan, and the Philippines. Social Science and Medicine 61: 2492–2500.
Bhagwati, J., and K. Hamada (1974). The brain drain, international integration of markets for professionals and unemployment: A theoretical analysis. Journal of Development Economics 1(1): 19-42.
Bhargava, A., and F. Docquier (2008). HIV pandemic, medical brain drain, and economic development in sub-Saharan Africa. World Bank Economic Review 22: 345-366.
Chauvet, L., F. Gubert, and S. Mesplé-Somps (2013). Aid, Remittances, Medical Brain Drain and Child Mortality: Evidence Using Inter and Intra-Country Data. The Journal of Development Studies 49(6): 801-818.
Kangasniemi, M., L.A. Winters, and S. Commander (2007). Is the medical brain drain beneficial? Evidence from overseas doctors in the UK. Social Science and Medicine 65: 915–923.
Lanati, M., and R. Thiele (2020). Aid for health, economic growth, and the emigration of medical workers, Florence: European University Institute, 2020 EUI RSCAS, 2020/104, Migration Policy Centre (MPC)
Moullan, Y. (2013). Can Foreign Health Assistance Reduce the Medical Brain Drain? Journal of Development Studies 49(10): 1436-1452.
Zelinsky, W. (1971). The Hypothesis of the Mobility Transition. Geographical Review, 61(2), 219-249. doi:10.2307/213996
Mauro Lanati , Research Fellow, Migration Policy Centre, EUI
Rainer Thiele, Director of the “Kiel Institute Africa Initiative” and adjunct professor of Economics at Kiel University
The EUI, RSCAS and MPC are not responsible for the opinion expressed by the author(s). Furthermore, the views expressed in this publication cannot in any circumstances be regarded as the official position of the European Union.